Back during the pandemic I did a number of posts looking at all-cause mortality in the USA. As a reminder, all-cause mortality is worth looking at because of the clarity of its definition. To give an example, if somebody has COPD and gets COVID-19 and dies, but probably wouldn’t have died if they only had one (then; COPD is eventually fatal), do you classify that as a COVID-19 death or a COPD death? Or as both? Different medical systems will reasonably differ on this question. (Then there are far less reasonable diagnostic criteria, like recording all deaths where a person had COVID-19 regardless of the cause of death.) This stuff can vary from hospital to hospital and state to state.
All-cause mortality data gets around these problems because, while it can be hard to agree on why a person died, it’s easy to agree on whether they died. Eventually. There is still the problem that it can take months for a death to actually be reported to the CDC. So much so that the CDC doesn’t even bother publishing all-cause mortality data for the most recently two weeks, and there’s very little point in looking at the last 3-6 weeks of data that they do publish. (They have algorithms that try to predict how many deaths will be reported eventually based on the data that has been reported so far, but it has a tendency to under-count what eventually gets reported.)
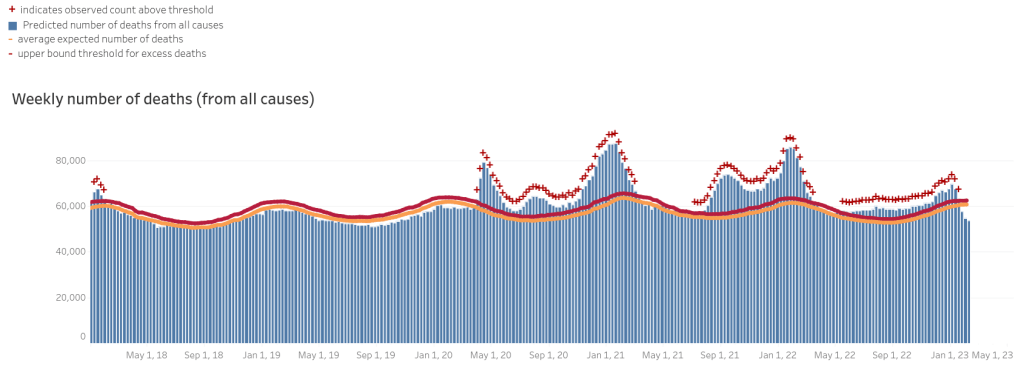
As I said, I put up several posts looking at this during the pandemic, and I recently became curious to look at it again now that the pandemic is in retrospect. So, here’s the data from the CDC as of February 20, 2023:
Let’s look at it a bit closer. To make the time frame of the data a little easier to follow, I’ve marked the approximate location of January 1 with yellow lines and the approximate location of July 1 with green lines:
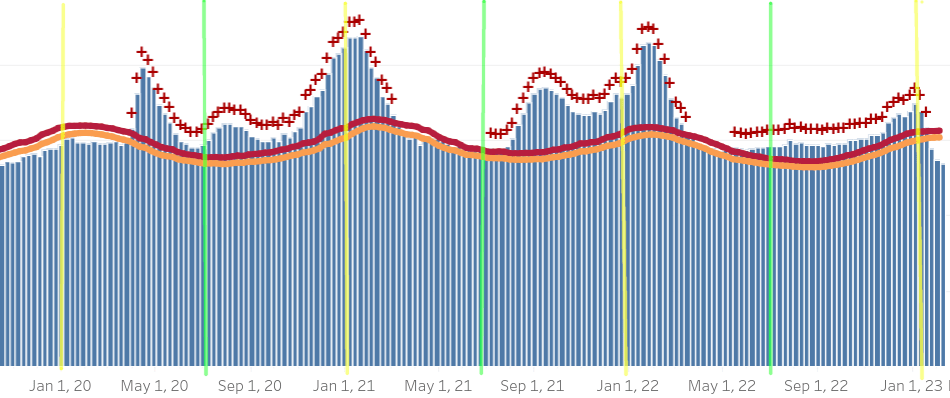
If you’re curious, the Pfizer vaccine received emergency use authorization in December of 2020. The more infectious Delta variant of SARS-CoV-2 was named in March of 2021. The Delta variant had mutations in the spike protein which is how the virus enters cells as well as the thing that the vaccine gives the immune system to detect. This simultaneously made it better at entering cells, and also reduced the efficacy of the immune response acquired through vaccination or infection with the original variant.
Because I sometimes would look at Sweden’s data, here’s their COVID-19 deaths/day as reported by the Swedish government:

This data is in no way directly comparable to the all-cause mortality data above, but it is none-the-less interesting to note how, with the exception of Summer 2020, the spikes like up pretty well. It is widely theorized that the US’s summer spikes correspond to air-conditioning season in the southern united states, when people stay indoors during waking hours. To the best of my knowledge, Swedish summers are far more mild than are the summers in the American south, so one would expect them to be absent.
That hypothesis brings up an interesting question looking at the USA data, though: why was there no summer spike in 2021? There was a spike in deaths in the fall of 2021, not the summer. One explanation is that COVID-19 deaths started taking longer since the onset of infection to kill people (or at least to contribute to their death). If that is the case we would expect all subsequent spikes in deaths to also come later and, indeed, they do. The winter spike in deaths (in early 2022) also came later than the spike in the winter of 2020/ 2021.
If that is the case, why should it be? One hypothesis which covers these facts—though is in no way certain—is that later mutations of SARS-CoV-2 took much longer to kill people than the original ones did. Another hypothesis which would explain the delay is that the most vulnerable people were killed off in the first waves, and everyone who is left are less susceptible. (Though they are less susceptible, it can still contribute to their deaths when they are weakened by other diseases.) These are just two hypotheses; the truth could involve some version of either, both, or neither.
Of course, another explanation which covers this data is that the response to the increases in prevalence of SARS-CoV-2, or very technically, the response to increasing numbers of positive SARS-CoV-2 tests, was responsible for the increase in deaths. This will, of course, vary among the states as they had very different responses to COVID; some states like California were known for draconian measures, while other states imposed very few restrictions, and many were inbetween. It is reasonable to suppose that the extra stress of lockdowns, closure of businesses, etc. would have some negative effect. There are no actions without consequences and it would be absurd to suppose that drastic actions like the ones taken in response to COVID-19 are free.
For reasons relating to other data I’ve looked into but don’t have time to get into here, I am skeptical that this explains all of the increase in mortality over the years before COVID, but I haven’t seen any data to conclusively rule that possibility out. I am also a bit resistant to this explanation because it would be too convenient; I think that the responses to COVID-19, after the first few months, were wildly overblown and a massive overreach of government power. Lockdowns could be justified in the face of a pandemic of the magnitude of the Black Death—something that could kill off a third of the population in a short time. During the very early rapid spread of SARS-CoV-2 there were reasons to believe that SARS-CoV-2 was an escaped bio-weapon that could have been that kind of threat—the kind of threat which could potentially justify temporarily suspending all of the normal rules of society. After a few months it was obvious that SARS-CoV-2, escaped bio-weapon or not, was in no way another Black Death. Since I think that what ensued as an unjustified massive overreaction, it would be very convenient if SARS-CoV-2 was barely worse than a normal flu and most of the bad consequences of it were actually due to what I consider to be an overreaction.
I like to be careful of convenient conclusions, especially when conclusive evidence is intrinsically hard to come by.
Whatever the cause and whatever exactly happened, it does seem very clear that it’s over. A few people still wear masks, but few enough that they might all be immuno-compromised people for whom trying to filter the air that they breathe in public places makes sense anyway. We still have some lingering excess mortality, though only slightly. It was never all that high—this is more clear when you look on a multi-year timescale rather than zooming in—and it is very possible that the last few years were a perfect example of Alexander Pope’s line, “a little learning is a dangerous thing.”
We had tests to detect the SARS-CoV-2 virus, but we didn’t know how it spread, how bad it was, or how bad it would be. Thirty years before, without the tests to detect the virus, the entire experience might have been radically different. The absolute worst weeks had increases in mortality of about 40%, but a 40% increase in a small number is still small. Throughout everything, there were only a few cases of hospitals becoming so over-full that they had to send patients elsewhere and there were no (or at least statistically no) instances of people dying because of a lack of treatment because the hospitals were full. Without the PCR tests that could detect the virus without symptoms (or with symptoms that could be a cold or the flu), and thus allow us to map out its spread, we might not have done much more than think that there was a nasty flu for a few years.
Discover more from Chris Lansdown
Subscribe to get the latest posts sent to your email.
